- Oct 18, 2023
Intraoperative Neuromonitoring for Urinary Bladder
- Faisal Jahangiri
- 0 comments

The urinary bladder is an important organ that serves the vital function of storing and emptying urine produced by the kidneys. The urinary bladder's innervation involves parasympathetic and sympathetic nerves, with precise coordination required between storage and voiding phases. Any injury to bladder innervation during complex pelvic or abdominal surgery can lead to urinary dysfunction postoperatively. Intraoperative neurophysiological monitoring (IONM) allows surgeons to identify at-risk nerves in real-time and take appropriate steps to preserve bladder function. This lecture will discuss the anatomy and physiology of bladder innervation, neuromonitoring techniques used during surgery, and their application in clinical practice to reduce complications.
Anatomy and Physiology:
The parasympathetic nerves that control the storage phase of the bladder originate from sacral spinal cord levels S2-S4. These sacral parasympathetic nerves travel inferiorly within the pelvis to innervate the detrusor muscle of the urinary bladder. Stimulation of these nerves causes contraction of the detrusor muscle and relaxation of the internal urethral sphincter, allowing urine to enter the bladder during storage.
The sympathetic nerves that control the voiding phase originate from thoracolumbar spinal cord levels T11-L2. These sympathetic nerves travel inferiorly within the pelvis and synapse onto the bladder neck, and trigone. Stimulation causes contraction of the internal urethral sphincter and relaxation of the bladder base and trigone, allowing controlled voiding of urine.
Precise coordination is required between the parasympathetic and sympathetic arms of bladder innervation to switch between storage and voiding phases. Sacral parasympathetic or thoracolumbar sympathetic nerve injuries can disrupt this balance and cause urinary retention or incontinence postoperatively. Neuromonitoring allows the identification of these at-risk nerves to help preserve bladder function.
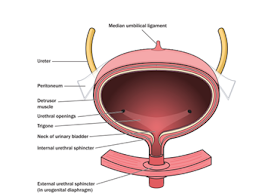
Figure: Cross-section through the urinary bladder, showing the detrusor muscle, ureters, and urethral sphincters (Jahangiri FR & Asdi RA, 2023).
Intraoperative Neuromonitoring:
Several techniques are used for neuromonitoring of bladder innervation during pelvic or abdominal surgery:
Urinary Sphincter Electromyography (EMG): Bipolar electrodes attached to the urinary catheter are placed to record external urinary sphincter (EUS) EMG. Electrical stimulation of sacral parasympathetic or thoracolumbar sympathetic nerves elicits a compound muscle action potential recorded by the electrodes. A drop in EMG response indicates nerve injury.
Anal sphincter EMG: Needle electrodes record the activity of the external anal sphincter muscle. Stimulation of sacral parasympathetic outflow causes detectable changes in anal sphincter tone. Loss of response indicates injury to sacral parasympathetic nerves.
Cystometry: A catheter is placed in the bladder and connected to a pressure transducer. Electrical stimulation of parasympathetic or sympathetic nerves causes changes in bladder pressure that are monitored. A loss of response suggests nerve injury.
Penile plethysmography: A mercury strain gauge is placed around the penis to detect blood volume changes during erection. Stimulation of pelvic splanchnic nerves causes increases in penile circumference that are monitored. Loss of response means nerve injury.
Nerve stimulation and mapping: Electrical stimulation allows localization of sacral parasympathetic and pelvic splanchnic nerves before they are at risk of injury. Their position is then avoided during dissection.
Clinical Applications:
Neuromonitoring helps reduce complications associated with pelvic surgery by allowing intraoperative identification of at-risk nerves supplying the urinary bladder. Some key clinical scenarios include:
Radical prostatectomy: Sacral parasympathetic stimulation helps identify the puboprostatic ligaments that can be safely cut without injuring the nerve bundle located laterally. Loss of EMG response warns of nerve injury, which can be immediately repaired.
Rectal cancer surgery: Pelvic splanchnic nerve stimulation identifies the nerve pathway medially in the pelvis. Sympathetic nerve injury can cause urinary retention so that the nerves can be preserved laterally.
Hysterectomy: Identification of sacral parasympathetic nerves as they course around the uterine vessels helps avoid injury, which could lead to post-operative urinary issues.
Aneurysmal repair: Thoracolumbar splanchnic nerves can be identified and preserved during aortic aneurysm clipping to avoid urinary dysfunction.
Sacral fracture fixation: Intraoperative monitoring helps identify sacral root injury from screw placement and allows technique modification to prevent postoperative bladder issues.
Cauda equina surgery: Intraoperative monitoring helps identify pudendal nerve injury during surgeries around the cauda equina to prevent postoperative bladder issues.
Tethered cord surgery: Direct nerve-triggered EMG helps identify the filum terminale and nerve roots. This helps to identify the lumbosacral nerves and prevent postoperative bladder issues.
Conclusion:
Neuromonitoring provides insights into neural functional integrity that cannot be obtained by visualization alone. It allows for identifying the nerves during the surgery and prevents any postoperative neurological deficits. Studies show that the intraoperative neuromonitoring teams who have more experience have much better postoperative outcomes.
References:
Jahangiri FR, Asdi RA, Tarasiewicz I, Azzubi M. Intraoperative Triggered Electromyography Recordings from the External Urethral Sphincter Muscles During Spine Surgeries. Cureus. 2019 Jun 10;11(6):e4867. doi: 10.7759/cureus.4867.
Jahangiri FR, Silverstein JW, Trausch C, Al Eissa S, George ZM, DeWal H, Tarasiewicz I. Motor Evoked Potential Recordings from the Urethral Sphincter Muscles (USMEPs) during Spine Surgeries. Neurodiagn J. 2019;59(1):34-44. doi: 10.1080/21646821.2019.1572375.