- Nov 3, 2023
Intraoperative Neurophysiological Monitoring of the External Urinary Sphincter During Spine Surgeries
- Faisal Jahangiri
- 0 comments

Surgery involving the lower spine and sacrum carries risks of damaging nerves responsible for lower urinary tract function. Injury to sacral parasympathetic nerves that control the bladder or pudendal nerves supplying the external urinary sphincter can result in urinary incontinence or retention postoperatively. Neuromonitoring of the external urinary sphincter allows surgeons to modify the technique in real-time to avoid iatrogenic nerve injuries during spine procedures. This blog will discuss the anatomy of external urinary sphincter innervation, techniques for intraoperative monitoring, and clinical applications in reducing complications associated with lower spine and sacral surgery.
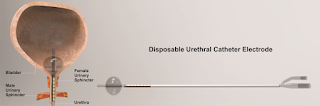
Figure: Urethral catheter Electrode: A disposable Foley catheter with embedded bipolar urethral catheter electrode contacts for electromyography (EMG) and transcranial electrical motor evoked potential (TCeMEP) recordings (Jahangiri et al., 2019).
Anatomy of External Urinary Sphincter Innervation
The external urinary sphincter (EUS) is a striated muscle located at the base of the bladder, which plays a crucial role in urinary continence. It receives motor innervation from the pudendal nerve, which originates from the S2-S4 nerve roots in the sacrum. After exiting the sacral foramina, the left and right pudendal nerves travel inferiorly through the Alcock's canal in the pelvis. They then give off perineal branches, which innervate the external urinary sphincter muscle.
Precise coordination is required between the external sphincter and the detrusor muscle of the bladder for continence. During urine storage, the sphincter remains contracted while the bladder relaxes. On voiding, the sphincter relaxes, allowing urine out while the bladder contracts. Any injury to the pudendal nerve branches risks disrupting this balance and causing urinary issues post-surgery.
Intraoperative External Urinary Sphincter EMG & TCeMEP Monitoring
In the past, needle electrode electromyography (EMG) was the main technique used for intraoperative monitoring of the external urinary sphincter. Fine wire electrodes were placed percutaneously into the sphincter muscle under vision. Recent development in electrodes has allowed us to use a urinary catheter with attached urethral electrodes for recording t-EMG, s-EMG, and motor-evoked potentials (TCeMEP) from the skeletal muscle of the external urethral sphincters. Electrical stimulation of the sacral roots, pudendal nerve, or perineal branches allows baseline EMG/TCeMEP responses to be recorded. Any reduction from baseline greater than 50-75% is considered significant and warns of potential nerve injury.
Stimulation can be applied during the surgical procedure, depending on the surgical exposure. Monitoring is beneficial during approaches near the sacrum, during rod insertion or fracture fixation, and when dissecting near the pudendal nerve pathway. It allows alteration of technique in real-time should a drop in t-EMG or TCeMEP response occur, reducing the risk of postoperative urinary issues.
Clinical Applications in Spine Surgery
Sacropelvic fixation: Fixation of pelvic or sacral fractures risks damaging sacral nerve roots, which supply the pudendal nerve. EMG monitoring guides rod placement and helps preserve sacral motor function to avoid new onset urinary symptoms.
Lumbar fusion: Dissection near the S2-S4 region or presacral spaces for interbody grafts carries a risk to pudendal innervation. Monitoring provides feedback on neural integrity during neural decompression and instrumentation.
Tumor resection: Sacral or presacral tumor removal, such as chordoma, presents challenges for sacral root and pudendal nerve preservation. EMG monitoring guides the extent of safe tumor removal.
Sacral laminectomy: Decompression of the cauda equina or conus medullaris requires excision of sacral lamina near sacral nerve root exit zones. Monitoring reduces the risk of iatrogenic root injury and urinary issues.
Disc herniation: Large lower lumbar disc herniations sometimes require a more medial decompression near the lumbosacral region. This poses a threat to the descending pudendal nerve pathway. EMG feedback assists in nerve identification and Avoidance.
Tethered cord release: Untethering the spinal cord presents challenges for sacral root and pudendal nerve preservation with a higher risk of associated lipomyelomeningocele. T-EMG monitoring guides the extent of safe tumor removal.
Outcomes and Advantages of EMG Monitoring
Numerous studies have found that intraoperative neurophysiological monitoring (IONM) during spine surgery significantly reduces new-onset postoperative urinary retention and incontinence. It provides dynamic feedback on neural functional integrity that cannot be obtained by static neural identification alone. Early injury detection allows immediate steps to prevent permanent harm. The key advantages are avoidance of lower urinary tract injury, reduced hospital stay and rehabilitation needs, improved patient quality of life, and lower medical expenditures overall.
In the field of neurophysiology, there have been two notable studies published that focus on monitoring the urinary bladder or external urethral sphincter (EUS) function using t-EMG (Jahangiri et al., 2019) and EUS-MEP (Jahangiri et al., 2019). These studies have shown promising results, particularly in surgeries involving nerve roots that supply the EUS. What makes these studies unique is that they are the first to demonstrate the possibility of monitoring motor-evoked potentials through EUS recordings, which is an added benefit to the already monitored EAS. This approach has the potential to significantly improve patient outcomes in surgeries that require a high level of precision and accuracy.
Conclusion
In summary, intraoperative external urinary sphincter monitoring is a valuable tool that spine surgeons can utilize to reduce complications affecting bladder function directly. It provides valuable insights into the functional status of sacral motor roots and pudendal innervation during approaches near this region. With appropriate application, neurophysiological monitoring helps optimize surgical outcomes.
References:
Jahangiri FR, Asdi RA, Tarasiewicz I, Azzubi M. Intraoperative Triggered Electromyography Recordings from the External Urethral Sphincter Muscles During Spine Surgeries. Cureus. 2019 Jun 10;11(6):e4867. doi: 10.7759/cureus.4867.
Jahangiri FR, Silverstein JW, Trausch C, Al Eissa S, George ZM, DeWal H, Tarasiewicz I. Motor Evoked Potential Recordings from the Urethral Sphincter Muscles (USMEPs) during Spine Surgeries. Neurodiagn J. 2019;59(1):34-44. doi: 10.1080/21646821.2019.1572375.