- Feb 20
Recurrent Laryngeal Nerve (RLN) Injury during Thyroid Surgery: Intraoperative Neurophysiological Monitoring as a Preventive Measure
- Heur Alass
- 0 comments
A person’s voice is their most personal and necessary communicative tool. To lose that is devastating and is an unfortunate reality for patients with recurrent laryngeal nerve (RLN) injury. This injury can be a postoperative complication due to thyroid-related operations, including complete thyroidectomy, which will be the focus of this exploratory piece. With varying statistics affected by circumstance, RLN injury is a serious and life-altering risk to a very common surgical procedure. Complete thyroidectomies are vital in cases of malignant and benign tumors, hormone disorders, and other health issues. They are performed out of necessity and are considered relatively safe, but the risk of nerve damage should be controlled as much as possible so that one health complication is not traded for another. The most important tool to combat this chance, even if relatively small per patient, is proactive preventive measures.
Thyroidectomies and the Recurrent Laryngeal Nerve
A thyroidectomy is the partial or complete surgical removal of the thyroid gland, a butterfly-shaped endocrine gland that sits in the front of the neck atop the trachea. Thyroidectomies have become one of the most common surgical procedures, having tripled in rate in the last thirty years. The total removal of the thyroid, known as complete or total thyroidectomy, has replaced many partial removal methods. These procedures are common for treating hyperthyroidism, removing goiter and thyroid cancers, and other hormonal or tumor-related conditions.
Understanding the Recurrent Laryngeal Nerve: Why It Matters in Thyroid Surgery
The recurrent laryngeal nerve (RLN) is one of the most important and most vulnerable structures encountered during thyroid and anterior neck surgery. A branch of Cranial Nerve X (the Vagus nerve), the RLN provides motor control to the intrinsic muscles of the larynx, allowing the vocal cords to open, close, and produce sound. Simply put, this small nerve plays a major role in breathing, speaking, and protecting the airway.
A Unique and “Recurrent” Pathway
The RLN earns its name from its unusual course. Rather than traveling directly from the Vagus nerve to the larynx, it first descends into the chest before looping back up toward the neck, hence the term 'recurrent'.
On the right side, the RLN loops under the right subclavian artery.
On the left side, it travels farther down, looping beneath the aortic arch, making the left RLN longer and slightly more vulnerable to thoracic pathology.
After looping, both nerves ascend through the tracheoesophageal groove to reach the larynx.
A Close Relationship with the Thyroid
From a surgical standpoint, the RLN’s intimate relationship with thyroid structures makes it especially challenging to protect:
The nerve is typically only about 2 mm in diameter, making it small and delicate.
It courses near the inferior thyroid artery, sometimes passing in front of it, behind it, or even between its branches.
It is frequently tethered near Berry’s ligament, a dense attachment of the thyroid gland to the trachea, an area where the nerve is relatively fixed and particularly susceptible to injury.
To complicate matters further, the RLN’s exact position can vary significantly between individuals, requiring careful identification rather than reliance on textbook anatomy.
Why Is the RLN at Risk During Thyroidectomy?
Because of its size, variability, and proximity to surgical landmarks, the RLN is vulnerable to several forms of intraoperative injury:
Traction or stretch during retraction
Compression or Contusion
Thermal injury from cautery devices
Transection during dissection
Even excessive handling can disrupt nerve function
These risks underscore why meticulous technique, and often intraoperative nerve monitoring, is used to safeguard the RLN.
Clinical Consequences of RLN Injury
Injury to the RLN can have profound functional consequences:
Unilateral injury often results in hoarseness, weak voice, or vocal fatigue due to paralysis of one vocal cord.
Permanent damage may lead to irreversible phonatory dysfunction.
Bilateral injury, though rare, is a surgical emergency. Both vocal cords can become immobile near the midline, potentially causing airway obstruction and acute respiratory distress.
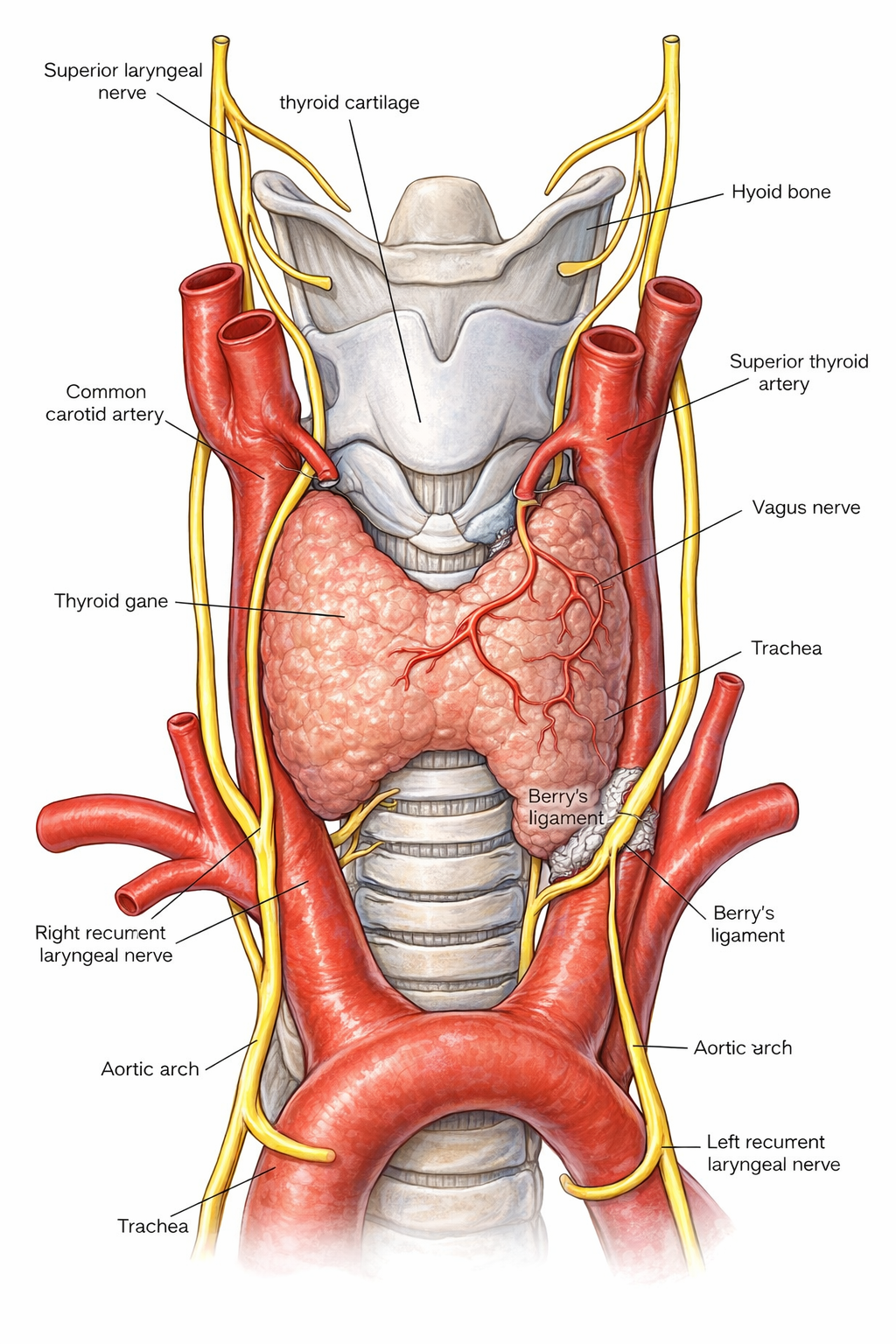
Figure 1. Anatomy of the recurrent laryngeal nerve and the superior laryngeal nerve.
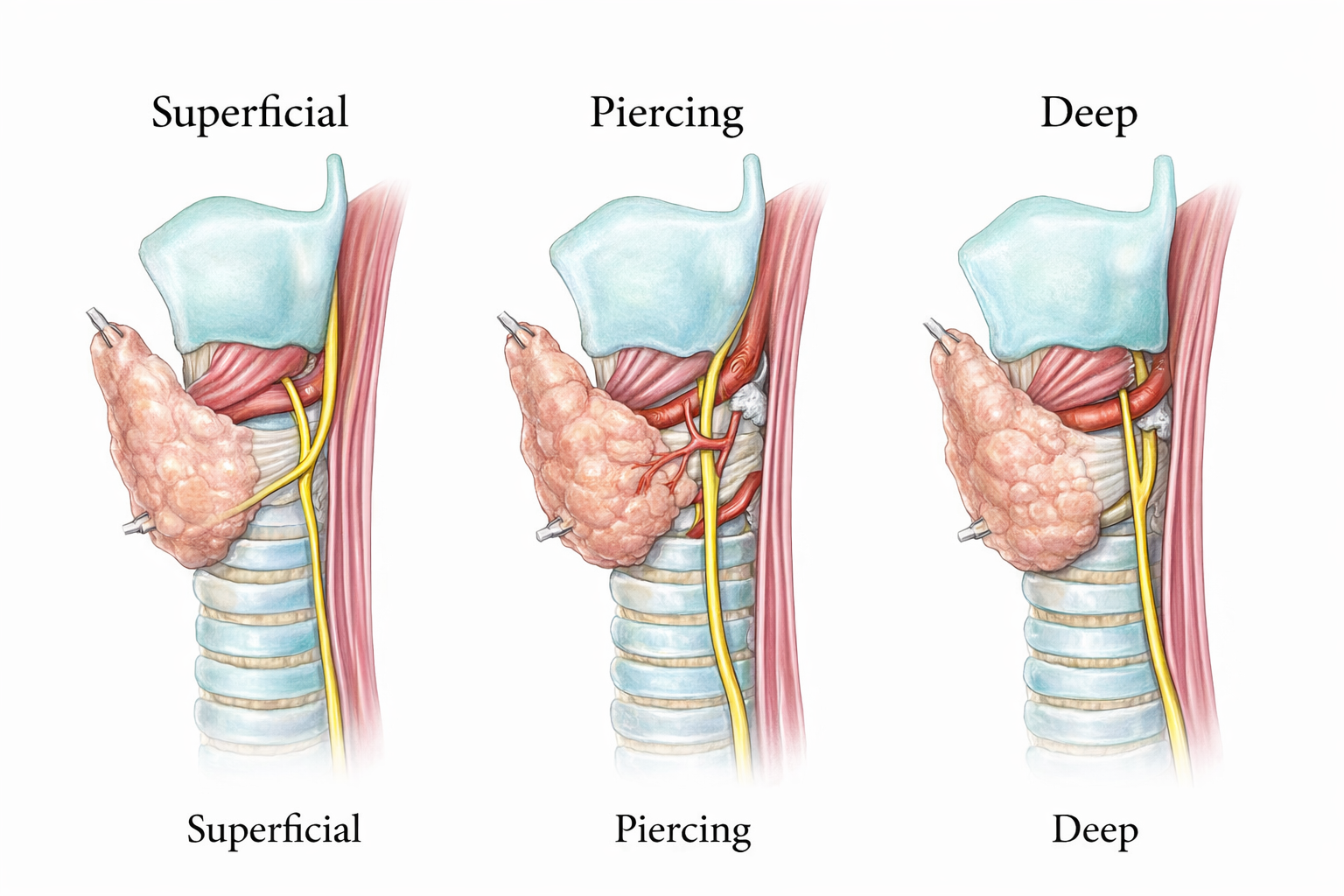
Figure 2. Types of relationship between the Recurrent Laryngeal Nerve and the Berry Ligament.
A Statistical Glance
While thyroidectomies are considered a safe procedure, statistics show a considerable amount of RLN injury-related complications. Various studies show different numbers, with one demonstrating that temporary RLN palsy occurs in 2-13% of cases and permanent RLN palsy in 0.4-5.2%. A review of 27 studies concluded that the average rate of RLN injuries from thyroidectomies was 9.8%, with the complication rate ranging between 2.3% and 26%. These large ranges result from many specificities that differ from case to case. Some patients have large tumors that can make the RLN harder to locate. Other patients may have larger goiters than others. Some patients may just have a more vulnerable RLN due to where it sits relative to the superior and inferior thyroid arteries. These differences affect RLN visibility to surgeons, thus affecting the possibility of traction or lesion to the nerve.
Prevention by Intraoperative Nerve Monitoring
Visibility of the RLN is the most important thing to decrease the possibility of injury. However, visibility does not tell the surgeon enough about the functional integrity of the nerve. This is where intraoperative nerve monitoring (IONM) plays a role. IONM continuously assesses the integrity and condition of neural tissues and structures, monitoring them and intervening early to prevent damage based on immediate feedback. In the case of the RLN, a study was conducted to compare 2556 patients who underwent total thyroidectomies: 1481 with IONM, and 1075 without. Results showed a significant 2.6% reduction (3.3% to 0.7%) of RLN injury incidence with IONM. While more studies are still being conducted to prove a significant reduction in RLN injury with IONM in general thyroid operations, it is most critical in high-risk thyroidectomies. In general, extra caution can be sacrificed during procedures considered safe. However, proactiveness with techniques such as IONM can truly make a difference for patients. For thyroidectomy patients, this preventative measure can save them from the possibility of a permanently lost voice, if not something more severe.
References
Choi, S. Y., & Son, Y. I. (2019). Intraoperative Neuromonitoring for Thyroid Surgery: The Proven Benefits and Limitations. Clinical and experimental otorhinolaryngology, 12(4), 335–336. https://doi.org/10.21053/ceo.2019.00542
Ghatol D, Widrich J. Intraoperative Neurophysiological Monitoring. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK563203/
Henry, B. M., Sanna, B., Graves, M. J., Sanna, S., Vikse, J., Tomaszewska, I. M., Tubbs, R. S., & Tomaszewski, K. A. (2017). The Reliability of the Tracheoesophageal Groove and the Ligament of Berry as Landmarks for Identifying the Recurrent Laryngeal Nerve: A Cadaveric Study and Meta-Analysis. BioMed research international, 2017, 4357591. https://doi.org/10.1155/2017/4357591
Vasileiadis I, Karatzas T, Charitoudis G, Karakostas E, Tseleni-Balafouta S, Kouraklis G. Association of Intraoperative Neuromonitoring With Reduced Recurrent Laryngeal Nerve Injury in Patients Undergoing Total Thyroidectomy. JAMA Otolaryngol Head Neck Surg. 2016;142(10):994–1001. https://doi.org/10.1001/jamaoto.2016.1954
Wojtczak, B., Sutkowska-Stępień, K., Głód, M., Kaliszewski, K., Sutkowski, K., & Barczyński, M. (2024). Current Knowledge on the Use of Neuromonitoring in Thyroid Surgery. Biomedicines, 12(3), 675. https://doi.org/10.3390/biomedicines12030675
Zakaria, H. M., Al Awad, N. A., Al Kreedes, A. S., Al-Mulhim, A. M., Al-Sharway, M. A., Hadi, M. A., & Al Sayyah, A. A. (2011). Recurrent laryngeal nerve injury in thyroid surgery. Oman medical journal, 26(1), 34–38. https://doi.org/10.5001/omj.2011.09