- Apr 3
How Intraoperative Neurophysiological Monitoring Is Transforming Surgery for Children With Cerebral Palsy
- Aisha Kazi
- ionm, neuromonitoring, neurophysiology, Blogs
- 0 comments
Introduction
How often do we take our daily movements for granted? Our ability to stand, walk, and control our limbs, we often view it as a guarantee rather than a privilege. However, for many children living with Cerebral Palsy (CP), a condition affecting 1 in 345 children (CDC Archive), those movements can be difficult, even impossible. A notable limitation is due to severe muscle stiffness, known as spasticity.
Physiologically, spasticity is a clinical outcome of an upper motor neuron lesion. In an individual with normal muscle tone, the muscles provide a small amount of smooth resistance when stretched. In a patient with spasticity, however, this resistance increases significantly. As a result, the patient’s movements are stiff and difficult to control (Chakravarty & Mukherjee, 2010).
This persistent muscle stiffness interferes with walking, balance, posture, and overall functional independence. Children with spastic cerebral palsy must expend significantly more energy to execute the same movements that many of us perform without a second thought. They must often rely on assistive devices, such as walkers, braces, wheelchairs, or extensive physical therapy to support mobility and daily activities. While these methods can help manage symptoms, some treatments aim to address the underlying neurological source, such as Selective Dorsal Root Rhizotomy (SDR).
Selective Dorsal Root Rhizotomy (SDR)
This neurological procedure aims to reduce spasticity in children with Cerebral Palsy, with many studies showing reductions in spasticity and improvements in mobility. A key distinction enables SDR to provide a significant improvement in quality of life compared to previous surgical techniques. Before the development of modern SDR, surgery consisted of severing entire dorsal sensory nerve roots within the spinal cord. While this method was successful in reducing muscle stiffness, it often resulted in significant weakness, loss of sensation, and, in some cases, paralysis (Park & Johnston, 2018). In other words, spasticity was reduced but often at a considerable cost. These complications adversely affect mobility and the child’s overall quality of life. As a result, more refined surgical techniques were developed. The key difference: severing specific nerves, rather than all of them. SDR surgery involves selectively cutting sensory nerve fibers in the lower spinal cord that are responsible for abnormal muscle signaling, specifically those that cause muscle tightness in the patient’s legs (Cleveland Clinic).
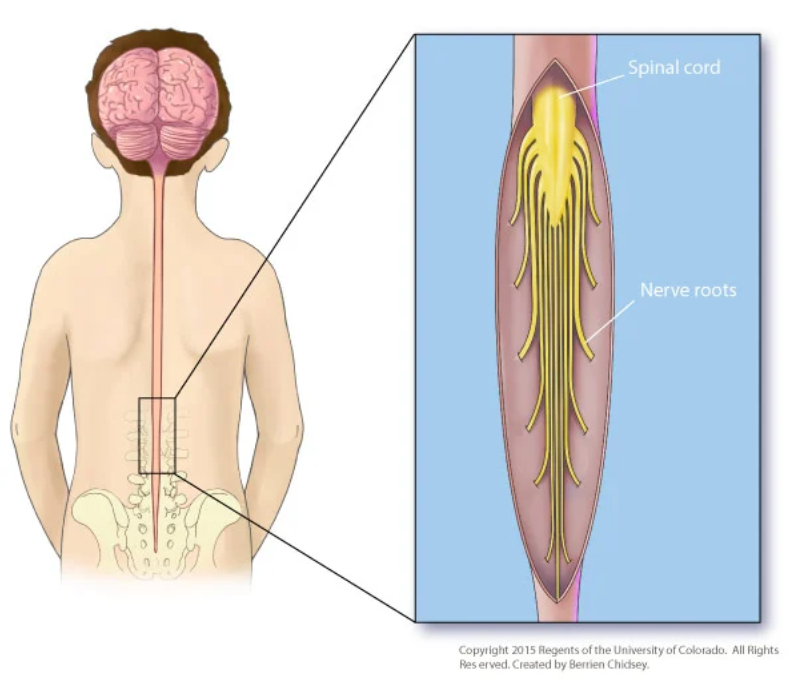
Figure 1. Anatomical overview of the spinal cord and dorsal nerve roots involved in SDR (Children’s Hospital Colorado).
A Deeper Look into Surgery with Intraoperative Nerve Monitoring (IONM)
The neurosurgeon begins by performing a small incision at the lower back, right above the waist, to access the patient’s spinal cord. To expose the spinal nerves, a portion of the lamina and spinous processes is removed. There is a natural anatomical separation between the sensory and motor nerves; ultrasound and X-ray imaging are used to locate the tip of the spinal cord, where this separation occurs. The sensory nerves are then divided into smaller rootlets before stimulation. While sensory nerves are being stimulated, motor nerves are monitored with Intraoperative Nerve Monitoring (IONM). Following a classic reflex pathway, the surgeon electrically stimulates a sensory (dorsal) nerve rootlet. The signal then travels into the spinal cord, entering the reflex circuit. If the pathway is abnormal, the leg muscles exhibit an exaggerated motor response. The rootlets are ranked on a spasticity severity scale, with 1 meaning mild and 4 meaning severe. The severely abnormal rootlets are then cut, and the technique is repeated (St. Louis Children’s Hospital).

Figure 2. A team of neurophysiologists is involved in Intraoperative Nerve Monitoring (IONM) of a Selective Dorsal Root Rhizotomy (SDR) procedure in the operating room.
The Positive Results
In a study following 85 patients over 27 years, the results show overwhelmingly positive outcomes following SDR surgery. With the addition of postoperative physiotherapy (PT), patients showed improved gait (walking pattern), functional independence, and self-care. The study followed up with adults who underwent SDR as children and reported sustained improvements and increased quality of life (Park & Johnston, 2018).
The evidence supporting both short- and long-term positive outcomes of SDR indicates that the procedure deserves its place among surgical innovations. The advantages of SDR over other procedures are numerous: reduced risk of spinal deformities, decreased motor weakness, and less intense back pain are just a few reasons why the technique is at the forefront of spasticity reduction in CP (St. Louis Children’s Hospital).
Intraoperative Nerve Monitoring (IONM) plays a critical role in the success of selective dorsal rhizotomy (SDR) surgery. IONM enhances surgical precision, setting it apart from traditional methods. By distinguishing between normal and abnormal nerve responses in real-time, IONM enables surgeons to preserve the essential nerve rootlets responsible for sensation and movement.
The outcomes of SDR can significantly restore movement in children with spastic cerebral palsy. With IONM involvement, surgeons can more accurately target the condition than ever before. Following SDR, patients often experience improvements in mobility, independence, and overall quality of life. These results represent not only significant surgical advancement but also the opportunity for patients to navigate the world with greater ease and confidence.
About the author:
Aisha Kazi is a senior neuroscience major at UT Dallas, preparing for medical school, currently balancing full‑time studies with part‑time work as a medical scribe and freelance tutor. Passionate about pediatric medicine, with strong skills in problem‑solving, time management, teaching, teamwork, and communication developed through academic, clinical, and volunteer experiences. Also proficient in creative tools, including Adobe After Effects, Photoshop, and Premiere Pro.Sources:
Centers for Disease Control and Prevention. (n.d.). Data and statistics for cerebral palsy. https://archive.cdc.gov/www_cdc_gov/ncbddd/cp/data.html
Chakravarty, A., & Mukherjee, A. (2010). Spasticity Mechanisms – for the Clinician. Frontiers in Neurology, 1, 7036. https://doi.org/10.3389/fneur.2010.00149
https://my.clevelandclinic.org/health/treatments/17458-selective-dorsal-rhizotomy
Park, T. S., Dobbs, M. B., & Cho, J. (2018). Evidence Supporting Selective Dorsal Rhizotomy for Treatment of Spastic Cerebral Palsy. Cureus, 10(10), e3466. https://doi.org/10.7759/cureus.3466