- Mar 12, 2024
Trapezius monitoring for Electromyography (EMG) and Motor Evoked Potentials (TCeMEP)
- Faisal Jahangiri
- 0 comments
The surgical anatomy of the Spinal Accessory Nerve (SAN) and the cervical plexus has been described in the literature. The exact motor innervation of the trapezius has been controversial due to variable motor innervation. The accessory nerve, when present, provides the most important input to the trapezius. Motor innervation from the cervical plexus is unpredictable but may be present in many patients. However, because of radicular overlap, limited sampling, confounding factors, and response variability, the effects range from no appreciable change to variable degrees of amplitude reduction to the disappearance, and some false-positive and false-negative results should be expected. Multichannel MEP recordings should span adjacent myotomes and avoid mixed myotome derivations for root monitoring.
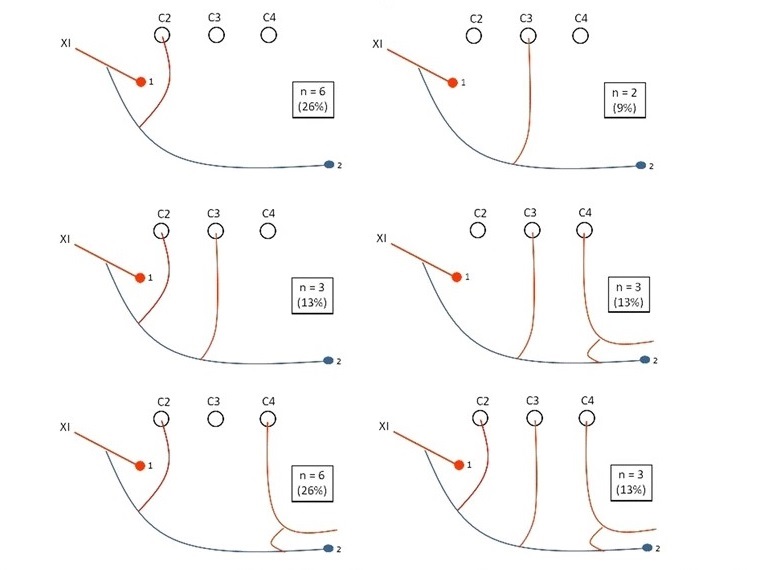
Figure 1. Schematic diagrams of anatomical anastomoses between the SAN branch running to the trapezius and the cervical plexus roots and their frequencies. 1 Indicates the SAN branch for the sternocleidomastoid muscle. 2Indicates the SAN branch running to the trapezius [1].
According to anatomy, the motor portion of the trapezius is innervated by the Spinal Accessory Nerve (CN XI), and the sensory portion is from C2-4. The most common cervical nerve root injuries reported are C5, C2 (during placement of C1 lateral mass screw), third occipital nerve (branch of C3), and C8 (during C7-T1 cervical osteotomy) nerve root injury. According to Gavid et al. (2016), the cervical plexus is not always involved in trapezius motor innervation, and the motor input from the cervical plexus to the trapezius muscle is provided in only 32 % of cases (Figure 1) [1]. In another study by Kim et al. (2014), the SAN provided the most consistent motor input to the trapezius muscle. The C2, C3, and C4 nerves also provided motor input to the trapezius muscle; however, they either needed to be more consistently present or, when present, irregularly innervated the three parts of the trapezius muscle [2]. Svenberg et al. (2015) reported that in 18/18 (100%) of the patients, the spinal accessory nerve (SAN) innervated all parts of the trapezius muscle (Figures 2 and 3). In 7/18 (39%) patients, an active motor branch from the cervical plexus was detected, equally distributed to all functional parts of the trapezius muscle, at levels comparable to the SAN [3].
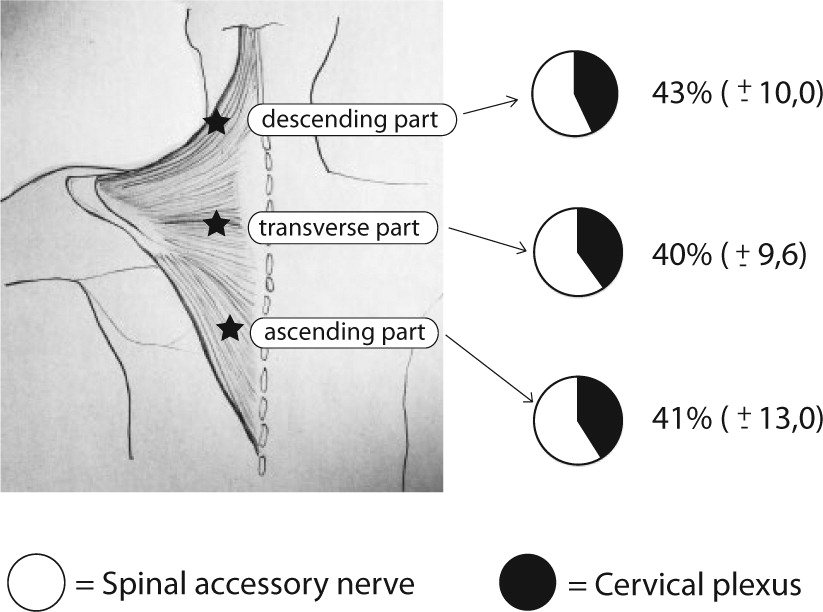
Figure 2. Relative neuromuscular function of the spinal accessory nerve (SAN) and cervical plexus in the three parts of the trapezius muscle [3].
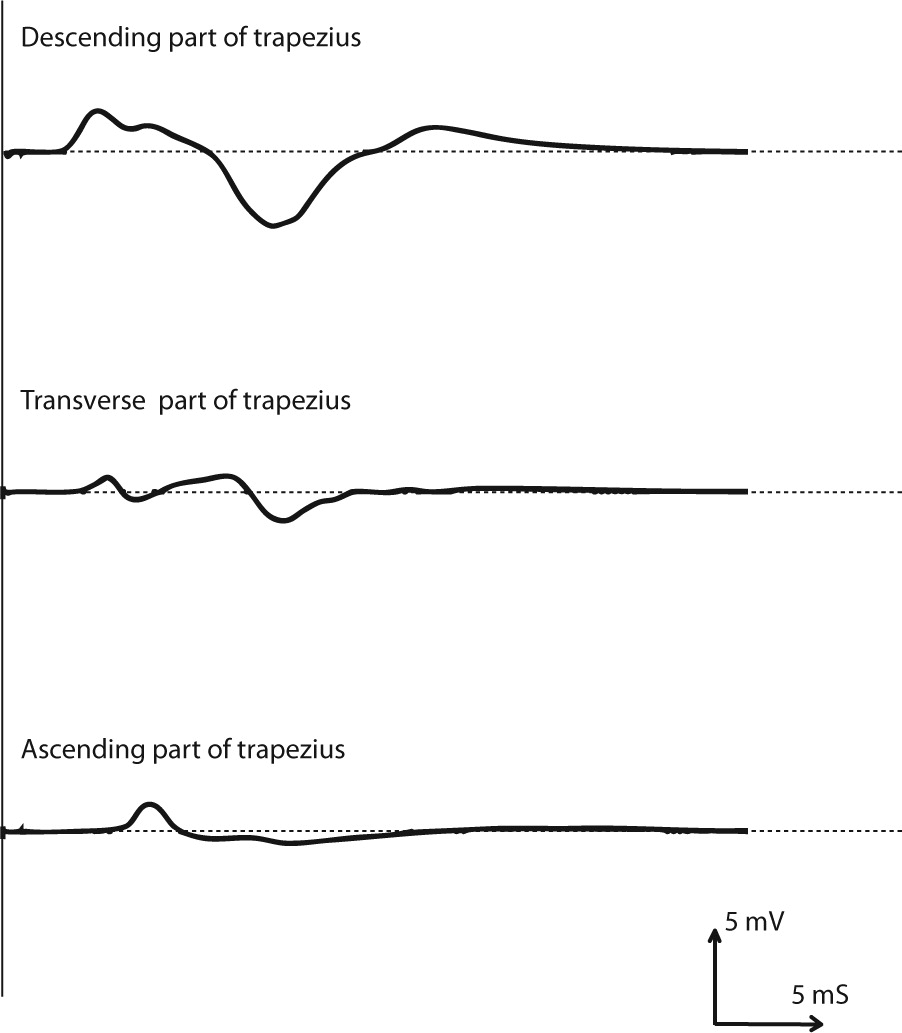
Figure 3. Compound muscle action potentials recorded from the descending, transverse, and ascending parts of the trapezius muscle following electrical stimulation of the spinal accessory nerve in a patient undergoing neck dissection. mV, millivolts; ms, milliseconds [3].
To minimize any false positive and false negative trapezius results, the cervical spine protocols should be updated in your recordings. You can create two protocols for all cervical spine cases, CERVICAL SPINE, and CERVICAL SPINE with TRAPEZIUS (in case the surgeon wants to monitor the Trapezius muscle). It is important to remember to place your electrodes in the trapezius muscle according to the surgery. Place electrodes in the upper trapezius to monitor the spinal accessory nerve for cranial nerve surgeries. Place your electrodes in the middle and lower trapezius to monitor the nerve roots with EMG or MEP. The motor supply is higher in C4 than in C3 and C2.
References:
Gavid, M., Mayaud, A., Timochenko, A., Asanau, A., & Prades, J. M. (2016). Topographical and functional anatomy of trapezius muscle innervation by spinal accessory nerve and C2 to C4 nerves of cervical plexus. Surgical and radiologic anatomy : SRA, 38(8), 917–922. https://doi.org/10.1007/s00276-016-1658-1.
Jin Hwan Kim, Kyu Young Choi, Kyu Ho Lee, Dong Jin Lee, Bum Jung Park, Young-Soo Rho; Motor Innervation of the Trapezius Muscle: Intraoperative Motor Conduction Study during Neck Dissection. ORL 1 May 2014; 76 (1): 8–12. https://doi.org/10.1159/000358923.
Svenberg Lind, C., Lundberg, B., Hammarstedt Nordenvall, L., Heiwe, S., Persson, J. K., & Hydman, J. (2015). Quantification of Trapezius Muscle Innervation During Neck Dissections: Cervical Plexus Versus the Spinal Accessory Nerve. The Annals of otology, rhinology, and laryngology, 124(11), 881–885. https://doi.org/10.1177/0003489415589365.